

5 Tests That Matter More Than BMI
One of the best predictors of illness is visceral fat, and standard labs usually miss it. Here is how we measure what’s actually happening inside your body.

UPDATED: February 15th, 2026
Welcome to the Beyond The Labs Newsletter, a weekly deep-dive into solving your health mysteries. I help adults in their 30s-50s solve the ‘Normal Lab’ mystery of brain fog, fatigue, and stubborn weight, to reclaim their energy and focus. I’m Dr. Ashori, a board-certified MD. I look Beyond the Labs through virtual Direct Primary Care in California and personalized health coaching for professionals worldwide.
The BMI is outdated. It often misses visceral fat, which is the only reason I care to know someone’s body composition. The BMI made it into the medical tool belt in 1972.
Body Mass Index (BMI) - The Crude Metric
Clinical medicine has evolved a lot in the past 53 years, making the BMI too crude for most of us. I came up with 5 far better tests that are far more informative.
Your weight fluctuates too much with stool and water retention/excretion, making it unreliable. Of course, on the extremes, your weight is quite important.
#1. Waist-to-Height Ratio
This is the best at-home test that predicts overall health. Measure waist at the narrowest point (or midway between ribs/hip crest), with a relaxed abdomen. Divide this number by your height in the same units.
I like this video from the NHS that shows you how to measure your WtHR.

#2. Mirror Test
I already wrote a newsletter on how to interpret the “mirror test”, but here is a brief summary.
1) Stand in front of a full-body mirror with good lighting.
2) From the front, look for waist indentation, love-handle fullness, and thigh/hip proportion.
3) From the side, look at abdominal shape. Soft fold you can pinch = more subcutaneous; a firm round belly you can’t pinch much = more visceral pattern.)
4) From the back, flank rolls and upper-back fat indicate more subcutaneous fat.

#3. DEXA Scan
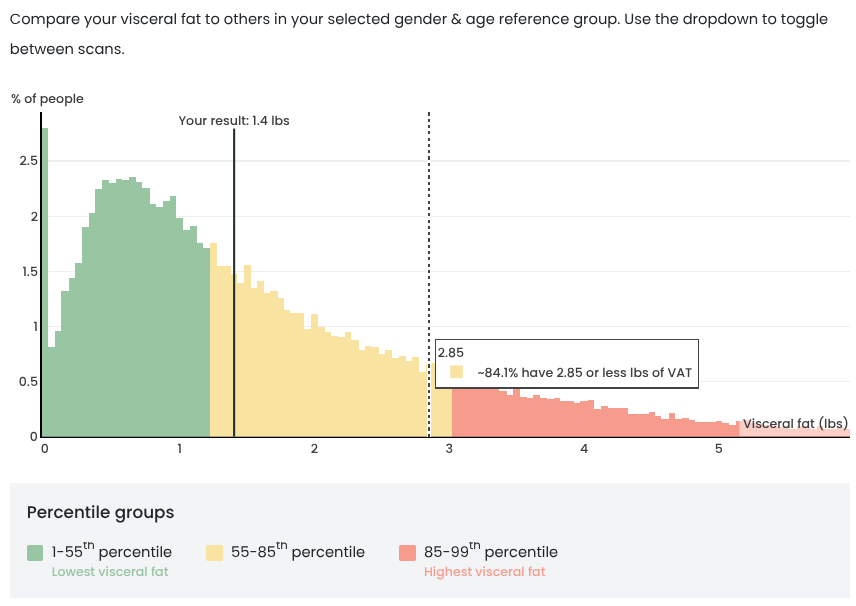
Modern DEXA scans can report not just bone density but muscle mass, fat mass, and differentiate between subcutaneous and visceral fat.
Though not as accurate as MRI, at around $100, it’s affordable and other than the slight radiation, it’s safe.
I’ve been using Body Spec because they have many mobile van units, which makes it convenient. You can check out their sample reports here.
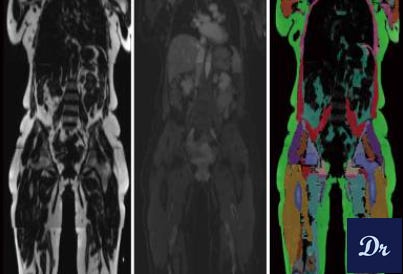
#4. MRI
This non-contrast MRI can cost anywhere around $250-500 and will show any visceral fat around the organs, and usually will include a PDFF (proton-density fat fraction) for fatty liver, specifically.
More most patients this is an unnecessary level of detail. But it’s one of the most accurate tests for visceral fat. When I still suspect visceral fat and DEXA is negative, I offer an MRI to those patients.
There are many websites where you can shop for direct-to-consumer radiology studies. I refer my own patients to websites like Radiology Assist or Green Imaging.
#5. Bioimpedance (BIA)
These scales come in many forms. Usually the ones with hand-grips tend to be a little more accurate.
At less than $100, these could be a good investment. Remember, this device is even more finicky than a DEXA, so your hydration status matters. They come with good instructions for all of that.

What Are Ideal Ranges & Values?
I realize that many “normal” results are listed but that’s not the way I do it in my health coaching practice.
Each person gets an individualized assessment and we interpret their results based on their individual risk. It would be a shame to have someone get their waist circumference in the ‘ideal’ range only to fail to address far more important risk factors.
Disclaimer:
Dr. Mohammad Ashori is a U.S.-trained family medicine physician turned health coach. The content shared here is for education and general guidance only. It is not personal medical advice, diagnosis, or treatment, and it does not create a doctor–patient relationship. Humans are complicated and context matters. Always talk with your own healthcare team before making medical decisions, changing medications, or ignoring symptoms. This information is to help you add more depth to those conversations.
I mean, yeah, I get it. But I’m nearing 60, have early onset dementia, and I’m otherwise healthy. Not overweight. Not thin. Maybe I’m a little depressed. I don’t know. Just pass me my brandy.
Really solid framing, Dr. Ashori, and I like that you’re treating BMI as what it is: a coarse proxy, not a physiologic truth. The emphasis on visceral fat as the clinically relevant signal (vs total weight) is exactly where preventive medicine is heading. 
Your “ladder” from accessible → precise is also practical:
1. Waist-to-height ratio as the best bedside screen (fast, free, behaviorally sticky). 
/. DEXA as an affordable next step that adds meaningful body comp context beyond the scale. 
3. MRI as the gold-standard-ish look at visceral + liver fat (PDFF), when someone needs true phenotyping. 
Two “yes, ands” that might strengthen this even further for readers:
1. If someone wants a cardiometabolic “tie-breaker” alongside body comp, pairing this with ApoB (or non-HDL-C), A1c/fasting insulin or OGTT/CGM, and BP often clarifies risk when body composition looks “fine” but physiology isn’t.
2. The “mirror test” is psychologically useful for some, but I’d keep emphasizing your core message: we’re not chasing aesthetics; we’re tracking risk and choosing the least invasive tool that answers the question.